Bardet Biedl syndrome and McKusick-Kaufman syndrome are often confused since there is an overlap of phenotype. I was presented a child with Bardet-Biedel syndrome initially treated as McKusick-Kaufman syndrome.
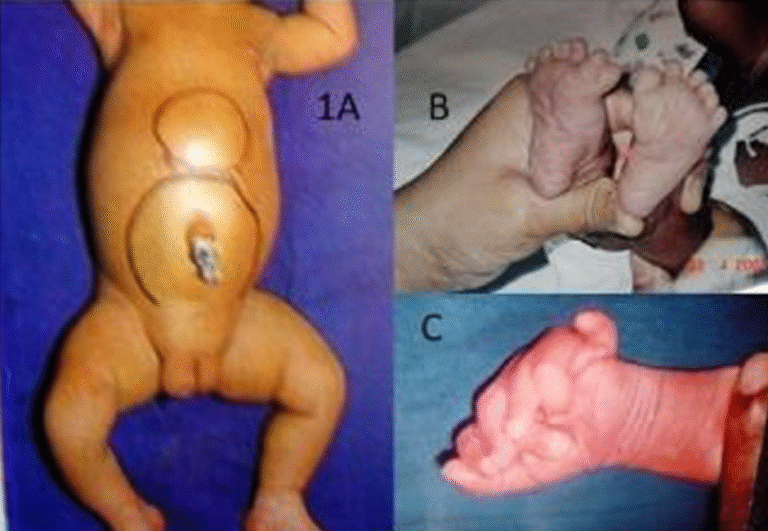
A new-born girl child was seen with lower abdominal swelling with postaxial polydactyly of both feet and left hand.
Clinically it was a suprapubic cystic swelling which persisted after the infant had voided the urine.
Clinical examination of the external genitalia showed an absence of vaginal orifice. The suprapubic swelling was hydrometrocolpos. A clinical diagnosis of McKusick Kaufman syndrome (MKKS) was made.
The ultrasound showed a grossly dilated vagina with debris containing fluid, the uterus was perched up over the dilated vagina.
Laparotomy was done. The grossly dilated vagina was decompressed. A Hegar’s dilator was pushed through the dilated vagina towards the place where a normal vagina would be present. Through a perineal incision, the vagina was dissected and vaginoplasty was done.
The child was followed up for a couple of years and the vaginal orifice was adequate.
The child was brought by the parents at eight years of age for review. The girl was obese with mental retardation and defective vision characteristic of Bardet- Biedl syndrome. Her brother had similar features with polydactyly.
Genetic testing could not be done due to financial reasons and both of them are being treated by us.
Bardet-Biedl syndrome (BBS) and McKusick-Kaufman syndrome (MKKS) are rare congenital disorders of autosomal recessive inheritance. Because of the phenotypic overlap of both
syndromes, including hydrometrocolpos postaxial polydactyly in the neonatal stage, the potential for diagnostic confusion exists.
In this case, the initial diagnosis was MKKS based on vaginal atresia, Post axial polydactyly. Later follow-up showed features of BBS with mental retardation visual problems and obesity. So, there is a significant clinical overlap between MKKS and BBS.